IN THIS ISSUE: ACLP President | Emergency Medicine | Delirium Webinar | Dlin/Fischer | What's New on the Web | CLP2024 | A&E Abstracts

Selection from the latest research impacting C-L Psychiatry
2024 ACLP Recommendations for Training Residents in Consultation-Liaison Psychiatry
Authors: Scott Beach, MD, FACLP, et al.
Despite rapid shifts in C-L Psychiatry training in residency, including increasing general residency training requirements from the Accreditation Council for Graduate Medical Education, greater utilization of advanced practice providers, and effects of the coronavirus pandemic, ACLP’s recommendations for residency training in C-L Psychiatry have not been updated since 2014.
A national survey of residency program directors in 2021 suggested many changes to the structure of C-L Psychiatry rotations at individual programs over the past decade.
The authors—a workgroup of eight ACLP members holding leadership positions in residency and fellowship education on local and national levels—reached 34 recommendations across four domains, including structural issues, faculty supervision, formal curriculum and evaluations, and elective experiences.
“These recommendations are intended to guide residency program directors towards optimizing C-L Psychiatry training for all residents, including those who will eventually pursue C-L Psychiatry fellowship,” say the authors. “Establishing a strong C-L Psychiatry foundation for all residents is essential for ensuring competency in providing psychiatric care for medically complex patients and collaborating with our colleagues in other specialties, as well as fostering trainee interest in pursuing a career in C-L Psychiatry.”
A summary of the recommendations across all domains is shown in Table 1 of the paper. Table 2 compares current recommendations with those of prior guidelines.
Importance: Training a psychiatric workforce with sufficient competence to manage patients with medical comorbidities, navigate complex systems of care, and collaborate effectively with non-psychiatrists is imperative for improving healthcare delivery.
Availability: Pre-publication in the Journal of the Academy of Consultation-Liaison Psychiatry (JACLP).

Advancing Measurement-Informed Care in Outpatient Community Behavioral Health
Authors: Deborah Scharf, PhD, et aL
Abstract: Measurement-informed care (MIC), also known as measurement-based care or patient-reported outcomes, for behavioral health conditions has had low uptake in the US.
To advance MIC, the authors reviewed nationally-endorsed behavioral health measures and worked with experts to recommend a core set of priority outpatient measures for use.
The resulting measures for common behavioral and comorbid conditions are outcome-based, low-burden, and suitable for value-based payment.
Behavioral health clinicians are urged to use repeated clinical measurements to improve outcomes and to support system needs by justifying, apportioning, and financing care. These practices align with those in chronic disease management in general medicine, in which measures such as hemoglobin A1c are used to determine diabetes care, and blood pressure is used to determine care for hypertension.
Collaborative care model research, showing that a single measure (i.e., the Patient Health Questionnaire–9) can inform primary care to enhance effectiveness and accountability in depression care, suggests that similar strategies may be effective in community behavioral health. Indeed, routine clinical measurements of behavioral health symptoms and other indicators (e.g., the therapeutic alliance) yield a range of benefits, such as improved client retention, reduced no-show rates, and improved clinical outcomes.
To realize their potential, however, behavioral health measurement approaches must also reflect the science, ideology, and culture of the field, say the authors.
Several recent reports direct clinicians and organizations toward a curated set of measures for their emerging measurement needs. “Although these proposed lists are helpful, stronger consensus is needed around a small core set of measures that can be broadly implemented and sustained,” say the authors. “Priority measures for this core set should be aligned with current population health recommendations for screening (i.e., by the US Preventive Services Task Force), widely endorsed quality measures (i.e., by the National Committee for Quality Assurance and Healthcare Effectiveness Data and Information Set), and measures with potential for broad use across the range of behavioral health populations and common comorbid conditions.”
Measures proposed by the authors are “meaningful across clinical and organizational purposes and are sustainable because of their low burden and benefits to patients, providers, payers, and regulatory agencies,” they say.
Their literature review here summarizes available quality measures endorsed by US national health care organizations between September 2022 and February 2023. They then review and code them along MIC-relevant dimensions, including diagnosis or disorder, population, psychometric properties, process versus outcome orientation, and specification of standardized assessment tools. Fewer than 25% of the >200 identified measures are patient-reported outcomes.
Twelve experts in addiction, administration, clinical care, integrated care, primary care, psychology, psychiatry, quality measurement, research, and social work reviewed the coded measure set. The primary issues they raised were the disconnect between regulators’, payers’, and general medical partners’ measurement expectations, and suitable measures for MIC in behavioral health.
The authors defined MIC as:
- Use of reliable and valid service user-reported outcomes or biometric indicators.
- Use of repeated measurements at clinically meaningful, regular intervals.
- Use of measure scores as one among other sources of information (e.g., service user preferences, social driver needs, culture, quality of life, functional needs and goals, family support, health literacy, and others) for making care decisions to support recovery.
- Use of the same measures to indicate accountability and efficiency of care.
Importance: MIC has the potential to improve behavioral health measurement uptake, implementation, and sustainability. Clinically, MIC may efficiently inform care and improve outcomes through effective use of data. Organizationally, a tightly curated and payer-aligned measure set can reduce burden from competing clinical, quality, accountability, and fiscal reporting practices. Aligned and synthesizable data sets can illustrate the impact of behavioral health services nationwide, which can help attract investment in behavioral health care.
Availability: Published by Psychiatry Online.

The Relationship Between Community-Based Psychiatric Rehabilitation Pathways and Re-Hospitalization Trajectories: A Three-Decade Follow-Up
Authors: Sharon Florentin, MD, et al.
Abstract: This study found:
- Use of psychiatric rehabilitation services for people with schizophrenia is associated with double time-to-readmission.
- People who use psychiatric rehabilitation services have lower mean annual rehospitalization days.
- More intensive residential services are associated with larger reductions in re-hospitalization days.
- Supported employment and sheltered workshops are the vocational services associated with the largest decrease in re-hospitalization days.
- Providing both vocational and residential psychiatric rehabilitation services has a synergistic effect on the reduction of re-hospitalization days.
Psychiatric rehabilitation is essential for the recovery of individuals with schizophrenia. However, re-hospitalization is sometimes inevitable. This study examines the association between varied community psychiatric rehabilitation services and long-term re-hospitalization parameters.
Data on 5,163 adults diagnosed with schizophrenia and schizoaffective disorder was studied. Patients with recurrent hospitalizations were tracked over three periods: before rehabilitation legislation (1991-2000), during rehabilitation implementation (2001-2009), and follow-up (2010-2017).
“Overall, community-based psychiatric rehabilitation service is linked to prolonged time-to-readmission and reduced re-hospitalization days,” say the authors. “A combination of vocational and residential services is related to a synergistic decrease in re-hospitalization days. This suggests that recurrent hospitalization for patients who are using psychiatric rehabilitation services is shorter and may be part of their recovery pathway.”
Importance: Over the years, the proportion of people who use residential or vocational psychiatric rehabilitation services has increased. This study examines the effect of using different types of psychiatric rehabilitation services, or none at all, on re-hospitalizations of people with chronic psychotic disorders who have a tendency to recurrent hospitalizations.
Availability: Published by Psychiatry Research.
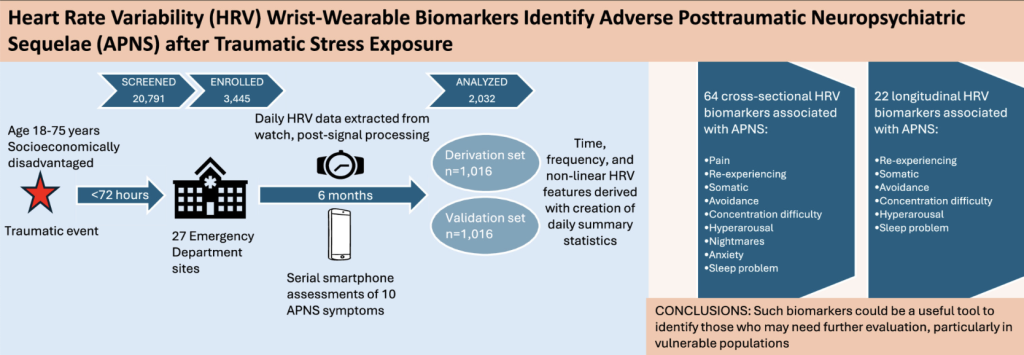
Heart Rate Variability Wrist-Wearable Biomarkers Identify Adverse Posttraumatic Neuropsychiatric Sequelae after Traumatic Stress Exposure
Authors: Lauriane Guichard, et al.
Abstract: Highlights of this study are:
- Heart rate variability biomarkers are associated with adverse symptoms post-trauma.
- Changes in heart rate variability biomarkers can predict adverse symptom worsening.
- Wrist-wearables may be useful as screening tools for adverse symptoms after trauma.
Adverse posttraumatic neuropsychiatric sequelae (APNS) are common after traumatic events. The authors examined whether wrist-wearables could provide heart rate variability (HRV) biomarkers for recovery after traumatic stress exposure in a large socioeconomically disadvantaged cohort.
Participants were enrolled in the emergency department within 72 hours of a traumatic event. Sixty-four characteristics were validated as cross-sectional biomarkers of APNS symptoms, including pain, re-experiencing, somatic, avoidance, concentration difficulty, hyperarousal, nightmares, anxiety, and sleep disturbance.
Many individuals who develop APNS after traumatic stress exposure go unidentified/undiagnosed. Select APNS symptoms are used in the diagnoses of acute stress disorder and post-traumatic stress disorder which are made at different time points after trauma, and these disorders include additional criteria such as the type of trauma and time elapsed since the trauma. Each individual diagnosis taken in isolation, however, may only partially capture the complexity of symptoms that occur after traumatic events.
Importance: There is increasing interest in leveraging data that can be collected from wearable devices to help identify individuals developing APNS. One type of measure is heart rate variability i.e., information that can be extracted from beat-to-beat variation in heart rate. More than one in five Americans wear a wrist-wearable device capable of collecting heart rate variability data.
Availability: Published by Psychiatry Research.
The Underuse of Clozapine and Long-Acting Injectable Antipsychotics
Authors: E. Fuller Torrey, MD, et al.
Abstract: In the US in 2019, the excess economic burden of schizophrenia, affecting approximately 3.9 million individuals, was $343.2 billion. This substantial cost “highlights the importance of effective strategies and treatment options to improve the management of this difficult-to-treat patient population,” say the authors.
Some patients do not have access to treatment; others do not respond to the treatments they receive. Still others do not adhere to treatment; for many, nonadherence is due to lack of insight into their illness and because they do not believe they are sick—i.e., they have a cognitive deficit called anosognosia.
The public face of this failure to appropriately treat schizophrenia includes approximately 100,000 homeless people with schizophrenia and related psychoses, and 200,000 incarcerated people with similar diagnoses.
Clozapine and long-acting injectable antipsychotics are among the most effective treatments, but both are markedly underused, say the authors.
The major reasons for the low use of clozapine are side-effects. Of primary concern is agranulocytosis, which requires monitoring with periodic blood testing. Myocarditis, seizures, and weight gain are other potential issues that contribute to patients’ reluctance to use the drug. The possible side-effects may also contribute to clinicians’ overestimation of patients’ reluctance to use clozapine and clinicians’ fears of legal liability, say the authors.
Importance: Clozapine became available in the US in 1989 and is the gold standard among antipsychotics. A meta-analysis reported that it is almost twice as effective as other antipsychotics. Clozapine is the only antipsychotic approved by the US Food and Drug Administration for decreasing suicidal ideation, has the lowest mortality rate among antipsychotics, and was reported to be more effective than other antipsychotics in decreasing hostility and aggression among patients with schizophrenia.
Despite its superior properties, only 4% of individuals treated with antipsychotic medication in the US receive clozapine, compared with rates of 20%-38% in countries such as Germany, Australia, Taiwan, and China.
Availability: Published by Psychiatry Online.